The list below is derived from clinical implications from the research findings described earlier:
Google.com
• Pick up, grasp and release objects of different shapes, sizes, weights,textures.
Google.com
• Hold and transport objects from one place to another.
Google.com
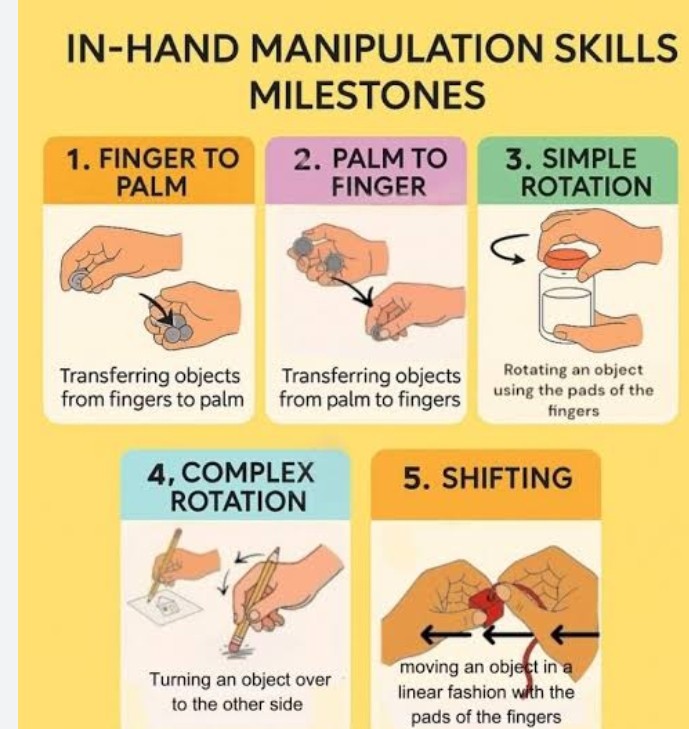
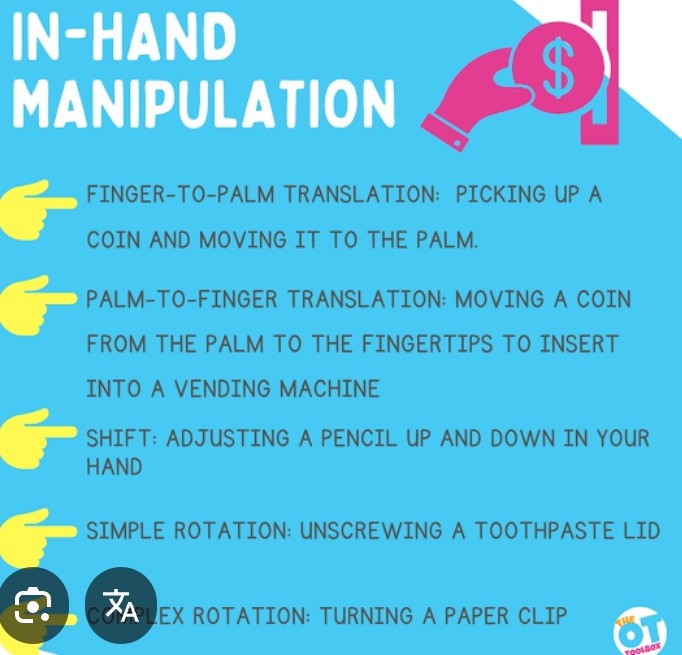
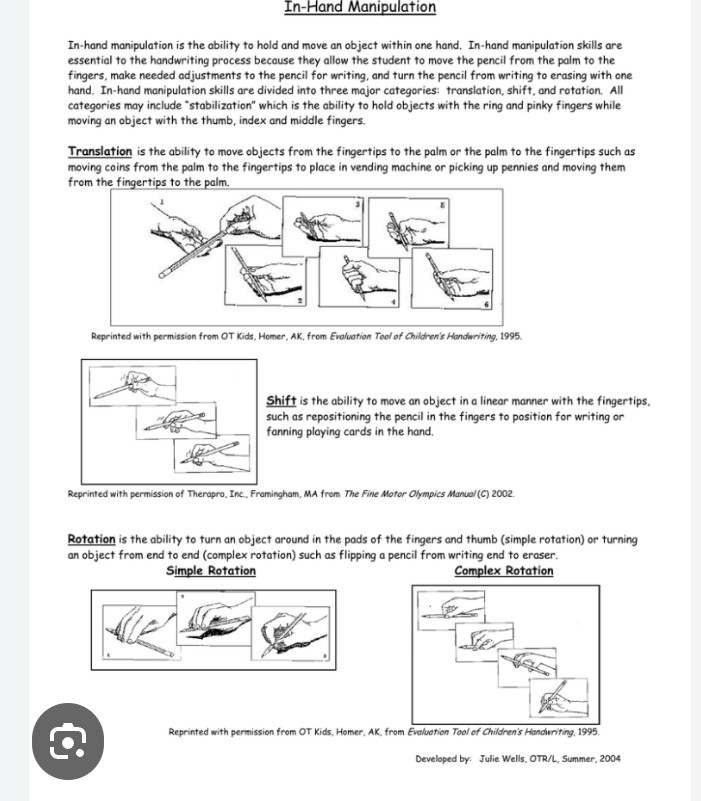
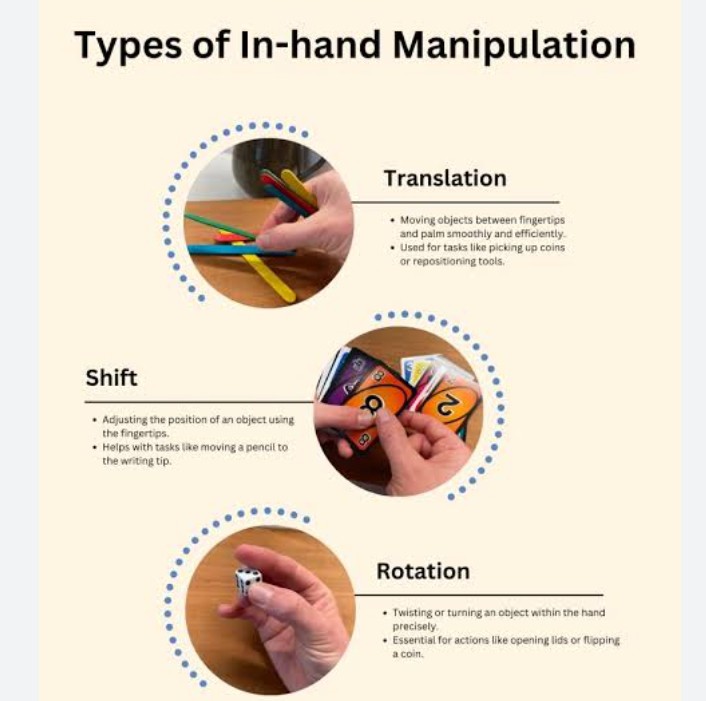
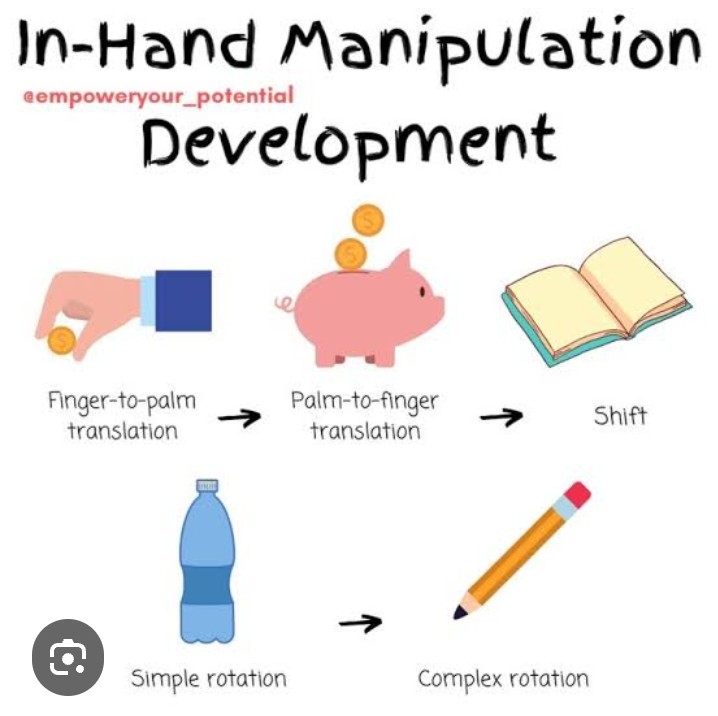
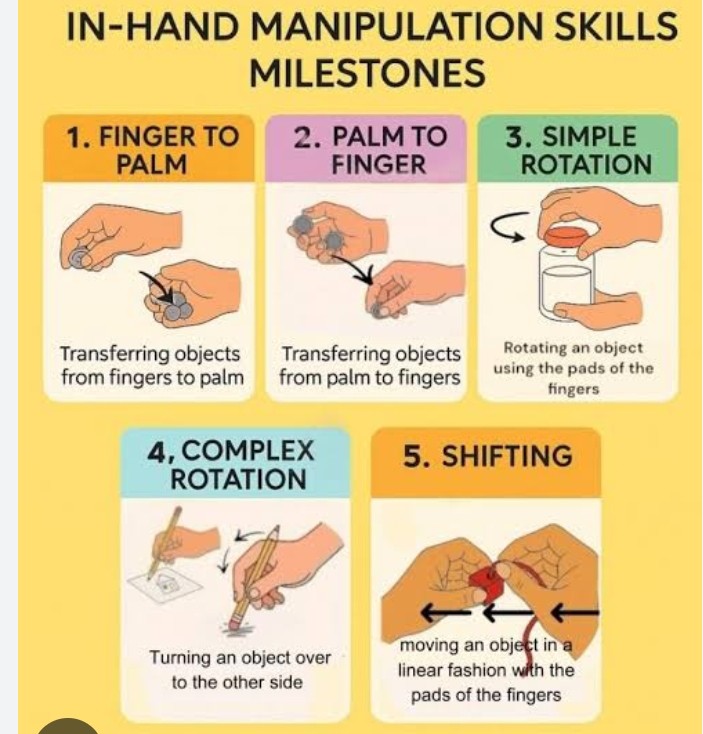
• Move objects within the hand.
Google.com
• Manipulate objects for specific purposes.
Google.com
• Reach for objects in all directions in sitting and standing.
Google.com
• Use two hands to accomplish specific tasks, e.g.one hand holding and the other moving (unscrewing lid of jar) – both hands doing the same movement (rolling out pastry) – each hand doing two different movements (peeling an apple).
• Throwing and catching actions to regain the ability to time action and to respond quickly to the ball.
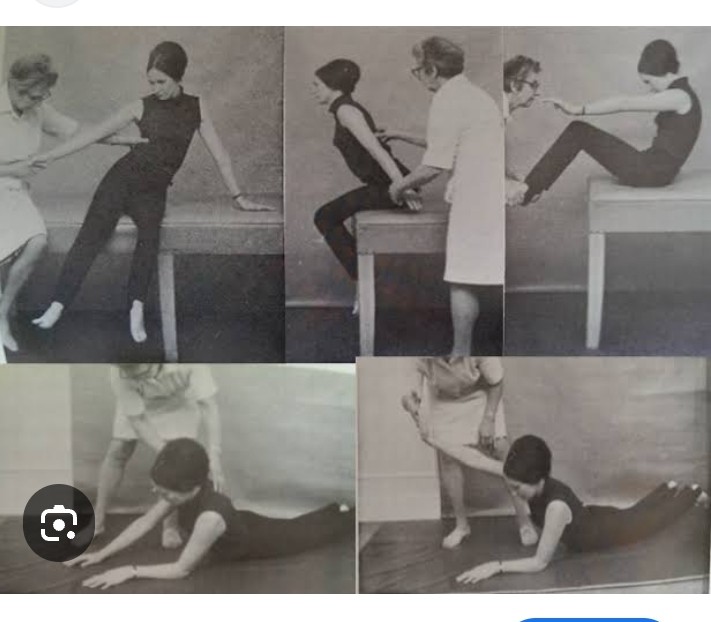
Head and trunk movements Sitting on a firm surface, hands in lap,feet and knees approximately 15 cm apart, feet on floor.
Turning head and trunk to look over the shoulder, returning to mid position and repeating to other side.
Check:
• Ensure patient rotates the trunk and head, with trunk erect, and remains flexed at the hips. • Provide visual targets, increasing the distance to be turned. • Stabilized the affected foot and prevent external rotation and abduction at the hip if necessary. • Ensure hands are not used for support and that feet do not move and Looking up at the ceiling and returning to upright.
Check:
• Patient may overbalance backward and is warned to keep upper body forward over the hips.
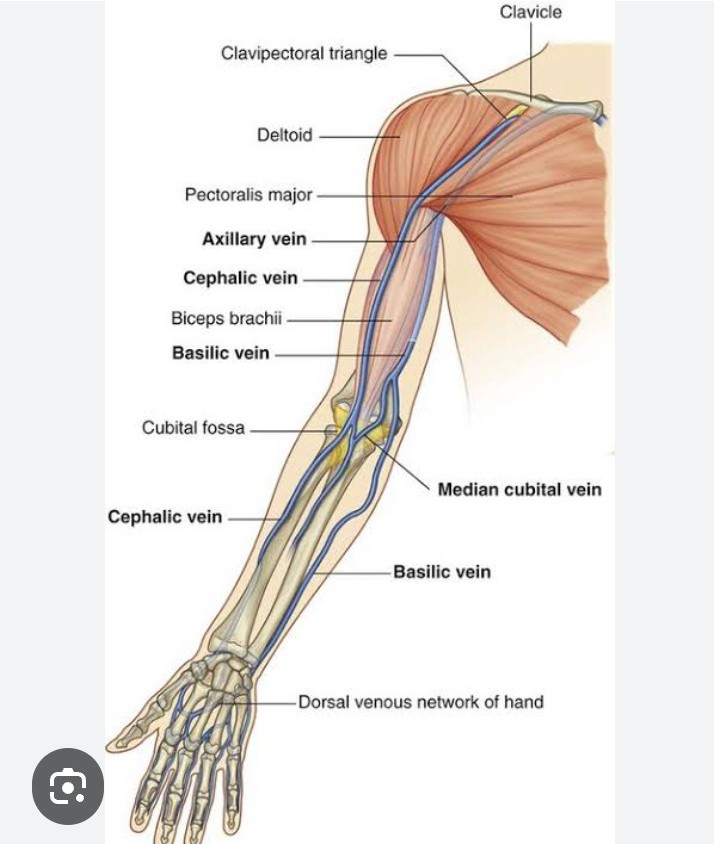
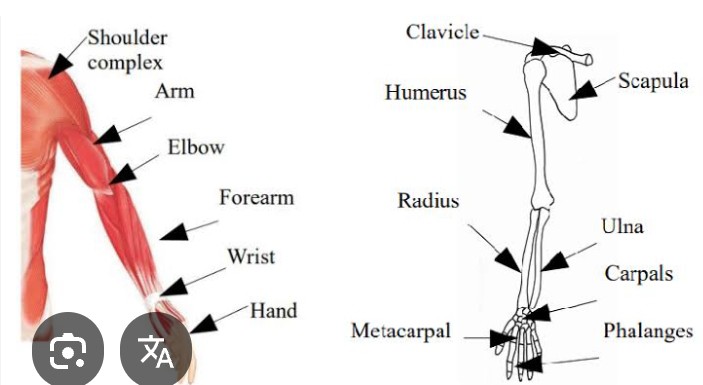
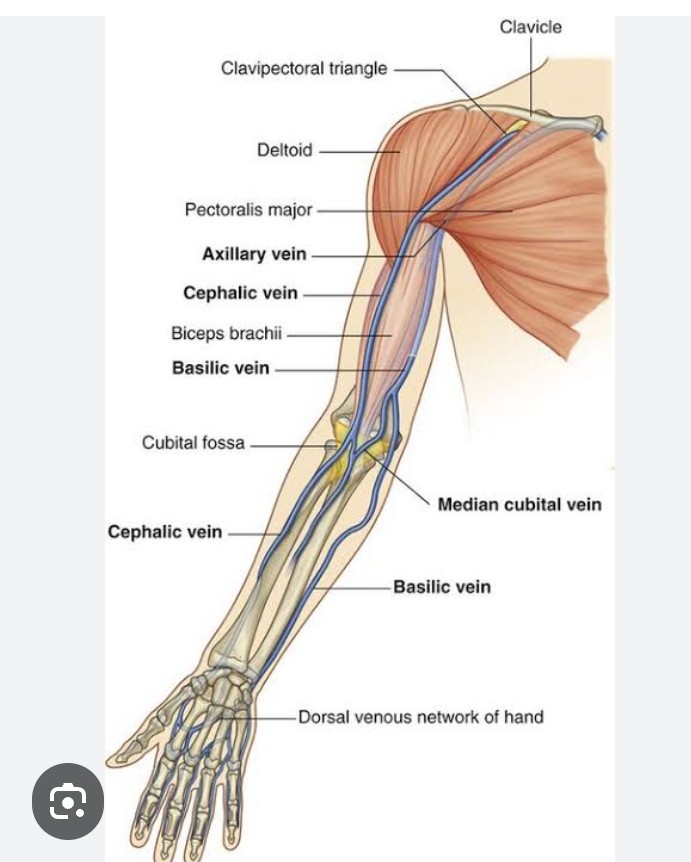
UPPER LIMB FUNCTION:
Training of muscle activity at the scapula and shoulder in supine until the patient can control his shoulder girdle in sitting without excessive compensatory movements.
Upper limb movement problems are usually secondary to shortening of soft tissues due to habitual posturing, use of the intact arm to compensate for the affected arm and learned non-use of the affected arm.
MANAGEMENT:
Early active mobilization of the affected arm in functional patterns.
CAUTION:
Soft tissue damage, chronic inflammation and joint stiffness may be caused by inappropriate passive exercises that do not accommodate the normal biomechanical relationship between the humerus and scapula.
Common Problems and Compensatory Responses:
Impaired scapular movement, especially rotation and protraction. Persistent depression of the shoulder girdle. Impaired control over the deltoids causing the inability to sustain shoulder abduction and flexion.
Compensation:
Excessive shoulder girdle elevation. Lateral trunk flexion. Excessive shoulder internal rotation,elbow flexion and forearm pronation. Weakness of glenohumeral joint (GHJ) abductors, flexors and external rotators and of supinators has a significant effect on reaching actions.
Weakness of wrist extensors, finger and thumb flexors and extensors,abductors and adductors affect the manipulation of objects.
Sustaining and controlling grip force during grasping and lifting objects is a common problem.
Reaching Actions:
Sitting,reaching to touch objects with the paretic hand: forward (flexing at the hips),sideways (both sides),backward, returning to mid position.
Very weak patients can practise reaching forward with arms resting on a high table.
Reaching forward: shoulder girdle elevation, lateral flexion of spine,abduction of shoulder with elbow flexion, internal rotation of shoulder and pronation of forearm.
• Pre-grasp:Excessive opening of hand for grasp to compensate.
• Releasing objects: finger extension with wrist flexed due to contracted long finger flexors,weak wrist extensors; extending thumb at carpometacarpal joint (CMC) and metacarpophalangeal joint instead of abducting at CMC.
Movement:
• Grasping: excessive flexor force in compensation for poor control. In addition, there are three common adaptive sequelae of stroke: • Use of the non-paretic limb preferentially when active movement is possible, and subsequent ‘learned non-use’ • habitual posturing of the paretic limb, leading to adaptive length-associated changes to soft tissues including loss of extensibility and increased stiffness of muscle.
Standing Balance:
Head and body movements Standing with feet a few cm apart, look up at ceiling and return to upright position.
Check:
• Ensure standing alignment is preserved, with hips extended while body rotates. • Disallow foot movement.If necessary put your foot against patient’s foot to stop movement.
Reaching actions:
• Correct tendency to fall back by a reminder to bring hips forward (hip extension beyond neutral) before looking up. • Disallow foot movement. Standing with feet a few cm apart, turn head and body mass and look behind,return to mid position, repeat to other side.
Check:
Standing, reaching to take object forward, sideways (both sides),backward.One hand, both hands.Variety of objects and tasks.Reaches should be beyond arm’s length, challenging the patient to extend the limit of stability and return.
Check:
• Ensure movement of body mass takes place at the ankles and hips, not just within the trunk. • Discourage a stiff posture and breath holding – encourage relaxed movement.
Single leg support (with or without harness or splint) Stepping forward with non-paretic limb to place foot on a step. Standing with either foot on step, practise reaching tasks.
Check:
• Ensure that the stance hip extends. Exercise can be practised initially in a harness. Note • Laufer et al. (2000) have shown that stepping forward on to a step of different heights with the non-paretic leg significantly increases weight borne through the paretic limb.
• The exercise directs attention to the concrete goal of raising the leg rather than the more abstract goal of shifting body mass.
Sideways walking:
This exercise enables practice of shifting weight from side to side with hips extended.
Google.com
Picking up objects:
Standing, lowering body mass to pick up or touch object, forward, sideways, backward and return.
Check:
• Ensure that hips, knees and ankles flex and extend. • Start with object on stool to minimize distance to be moved (see Fig. 2.17c). • Increase flexibility by changing base of support.
Action Reaching :
Forward: flexion at GH joint*
Sideways: abduction at GH joint*
Backward: extension at GH joint* with – elevation of shoulder girdle – external rotation at GH joint – extension of elbow – supination and pronation of forearm – extension at wrist
Grasping:
Extension of wrist and fingers, with abduction and conjunct rotation (‘opposition’) of the CMC joint of thumb and 5th finger. Flexion of fingers and thumb around object.
Releasing:
Extension at wrist. Extension at MCP joint of fingers. Abduction and extension at CMC joint of thumb.
Manipulation:
Flexion and extension of MCP joints of fingers with wrist in extension.
Google.com
Palmar abduction and conjunct rotation of CMC joint of thumb. Combined flexion and conjunct rotation at CI”IC joints of 5th finger and thumb (e.g. cupping) Independent finger flexion and extension (e.g. tapping)
Key grasp configurations, for example thumb-index; thumb-5th finger; 4th, 5th finger into palm; thumb + flexed MCP, extended interphalangeal (IP) joints of fingers (paper-holding grasp)
Foot placement. Forward trunk inclination by hip flexion with the neck and spine extended. Hip extension (for final standing adjustment)
ESSENTIAL COMPONENTS OF SITTING DOWN:
Forward trunk inclination by hip flexion with the neck and spine extended. Knee flexion
Common Problems:
Inability to shift the center of gravity forward sufficiently during the early stages of standing up and the late stages of sitting down. Failure to place the affected foot.
Common Compensatory Responses:
Weight borne primarily on the intact side which becomes accentuated when the intact foot is positioned posterior to the affected foot.
Forward neck and trunk flexion or wriggling forward to the edge of the chair to shift the weight forward.
SPECIFIC TECHNIQUES:
To Stimulate Trunk Inclination Forward at the Hips Practice Standing Up Practice Sitting Down.
BALANCED STANDING:
Appropriate body alignment Correct adjustments made to changes in body alignment (with shifts in the center of gravity).
Increases awareness of bilaterality,position in space and positioning of body parts; may minimize the development of spasticity.
BALANCE:
Constant accurately balanced movement of the center of gravity on a stationary base to keep the line of gravity just in front of the ankles.
Standing without using undue muscle activity, to move about in standing, to move in and out of the standing position, and to walk without arm support.
Description of Normal Function:
ESSENTIAL COMPONENTS OF STANDING ALIGNMENT:
Feet a few inches apart Symmetrical weight-bearing. Extended knees and hips Hips over feet Erect trunk. Shoulders over hips Head balanced on level shoulders.
ESSENTIAL COMPONENTS OF BALANCE REACTIONS:
Lateral shift in the center of gravity Lateral neck flexion. Lateral trunk flexion (pelvic elevation, shoulder depression) Backward shift in the center of gravity. Neck extension Forward trunk inclination at the hips. Ankle dorsiflexion.
WHAT TO DO…
Observe standing alignment Test the ability to adjust to self-initiated movement of head, trunk and limbs. Looking behind, up Grasping an object from the floor. Standing on one leg Reaching in various directions. Test the displacement of weight sideways and backward (equilibrium reactions) with feet a few inches apart.
Google.com
Common Compensatory Responses:
Wide base of support (placement of the feet and knees apart) Voluntary restriction of movement (holding the breath or maintaining a stiff body posture) Shuffling of the feet instead of adjusting using appropriate body segments. Stepping sideways or backward as soon as the center of gravity moves. Leaning backwards when the center of gravity shifts sideways Proximal (instead of distal) movement of parts when shifting the center of gravity.
Use of protective support by the upper limbs (grabbing for support, holding arms out sideways or forward) with minimal shifts in the center of gravity.
SPECIFIC TECHNIQUES:
To Stimulate Hip Extension To Maintain Knee Extension To Stimulate Adjustments to Shifts in Center of Gravity.
To Stimulate Essential Aspects of Balanced Standing Alignment. To Stimulate Protective Support through the Arm.
(AMBULATION WILL BE DISCUSSED AND COMPARED WITH PERIPHERAL NEURO-MUSCULAR FACILITATION AND THE NEURODEVELOPMENTAL TECHNIQUES)
Following are the mentioned Essential Components -MRP of Upper Limb:
Google.com
1.SITTING UP FROM SUPINE:
Rolling over to and sitting up from the intact side in the early stages of stroke,is given minimum period for practice.
Description of Normal function:
Essential components of Rolling:
Onto the side Neck flexion and rotation Shoulder flexion and protraction Trunk rotation Hip and knee flexion Other components: posterior hip shifting; foot pushing on the bed
Essential components of Sitting:
Up over the side of the bed Lateral neck flexion Lateral trunk flexion Lowering of the legs over the side of the bed
Other component: Shoulder abduction of the lower arm
Common compensatory responses:
Forward neck flexion and rotation Pulling self over using the intact hand; wriggling Hooking of the intact leg under the affected leg to dangle over the side of the bed Specific techniques To stimulate shoulder girdle protraction for rolling over
To stimulate hip extension for rolling onto the side To stimulate lateral neck flexion.
Google.com
2.BALANCED SITTING:
Appropriate body alignment Correct adjustments made to changes in body alignment (with shifts in the center of gravity).
BALANCE:
Sitting without using undue muscle activity, to move about in sitting, to move in and out of the sitting position, without arm support.
BALANCE REACTIONS:
Head trunk and limb movement in response to any shift in the center of gravity to maintain balance.
Protective extension only occurs when the center of gravity is moved so far that balance is lost.
Description of Normal Function:
3.ESSENTIAL COMPONENTS OF SITTING ALIGNMENT:
Feet and knees close together Symmetrical weight-bearing / sitting Hip flexion with trunk extension Head balanced on level shoulders
ESSENTIAL COMPONENTS OF BALANCE REACTIONS:
Lateral shift in the center of gravity. Lateral neck flexion Lateral trunk flexion (pelvic elevation, shoulder depression) Backward shift in the center of gravity. Forward neck and trunk flexion.
WHAT TO DO…
Observe sitting alignment Sitting on a firm base with feet flat on the floor, knees and feet a few inches apart and hands on the lap.
Test the ability to adjust to self-initiated movement of head, trunk and limbs.
Looking behind, up Grasping an object from the floor.
Lifting the intact leg and foot.
Reaching in various directions Test the displacement of weight sideways and backward (equilibrium reactions) .
Common Compensatory Responses:
Wide base of support (placement of the feet and / or knees apart) Voluntary restriction of movement (holding the breath or maintaining a stiff body posture) Shuffling of the feet instead of adjusting using appropriate body segments Leaning forward or backward when the center of gravity shifts sideways Use of protective support by the upper limbs (grabbing for support, holding arms out sideways or forward) with minimal shifts in the center of gravity.
SPECIFIC TECHNIQUES :
To Stimulate Adjustments to Shifts in Center of Gravity.
To Stimulate Essential Aspects of Balanced Sitting Alignment.
4.STANDING UP AND SITTING DOWN:
Placement of the feet and shifting of the body such that the center of gravity moves forward or backwards Good sitting balance is not a prerequisite to standing up; the patient, however, needs good sitting alignment.
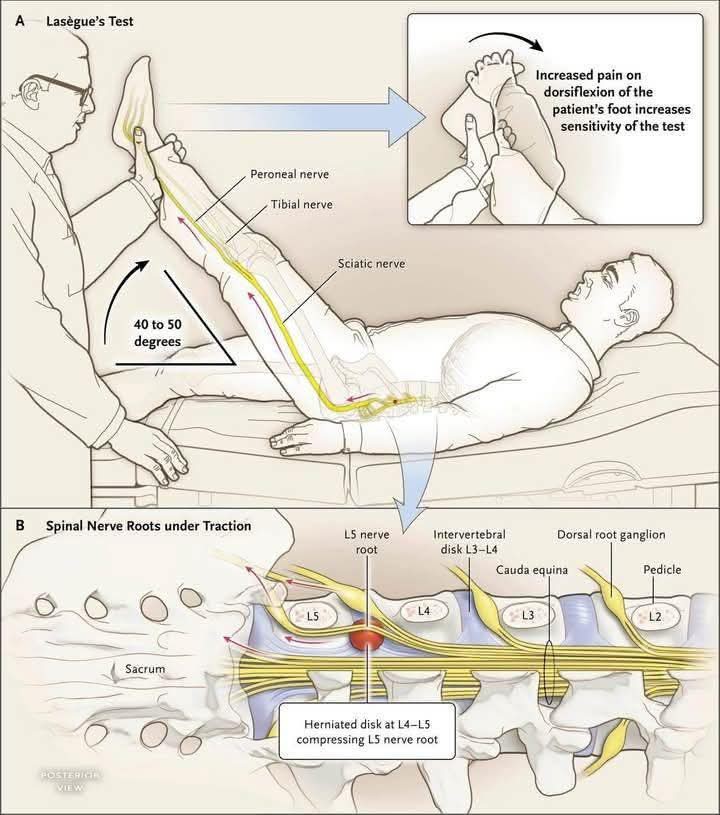
The terms “Lasegue test” and “straight leg raise test” are synonyms or being used interchangeably for the same physical examination maneuver used to assess nerve root irritation in the lower back.
It involves passively lifting a patient’s leg with the knee straight to see if it causes pain that radiates down the leg, which can indicate conditions like a herniated disc.
There are no differences between the two names.
Google.com
Lasegue Test /Straight Leg Raise (SLR) Test:
Purpose:
To check for nerve root irritation in the lumbosacral area, often caused by a herniated disc or other nerve compression.
Procedure:
The patient lies down while the examiner lifts their straight leg to flex the hip.
Positive sign:
The test is considered positive if pain radiates down the leg, particularly between (35 degree and 70 degree) of hip flexion, which suggests nerve root tension.
Additional Assessment:
The examiner may then have the patient flex or point their foot (dorsiflexion) to see if the pain worsens, which can help confirm the diagnosis.
Historical context:
The test is named after Dr. Charles Lasegue, but it is believed that Dr. Lazar Lazarevic was the first to describe it.