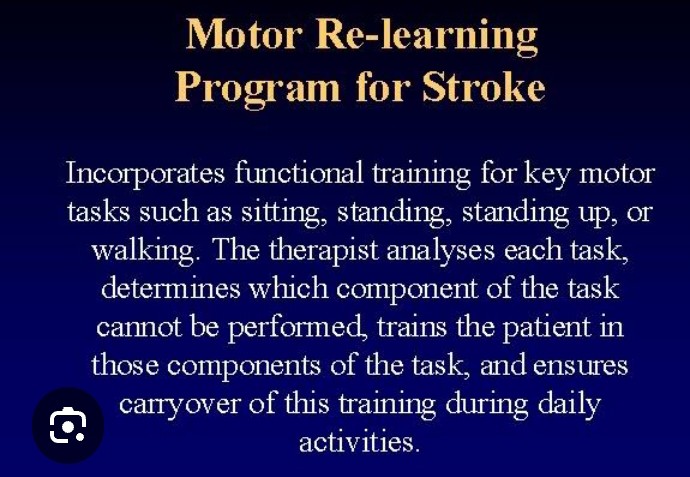
1. ANALYSIS OF TASK:
Observation as the patient performs (or anticipates to perform) the activity.
Note: Any missing components
Incorrect timing of components within a movement pattern.
Absence of specific muscle activity.
Presence of any excessive or inappropriate muscle activity.
Compensatory motor behaviour,selection of essential movements upon which the activity depends:
Selection of the most essential components if many components are missing (i.e., the patient is barely able to move)
2. PRACTICE OF MISSING COMPONENTS:
Practice at peak performance for at least 30-60 minutes or more twice daily; progression when some form of control is seen.
Switching from verbal instruction to visual demonstration or vice versa if a person does not respond.
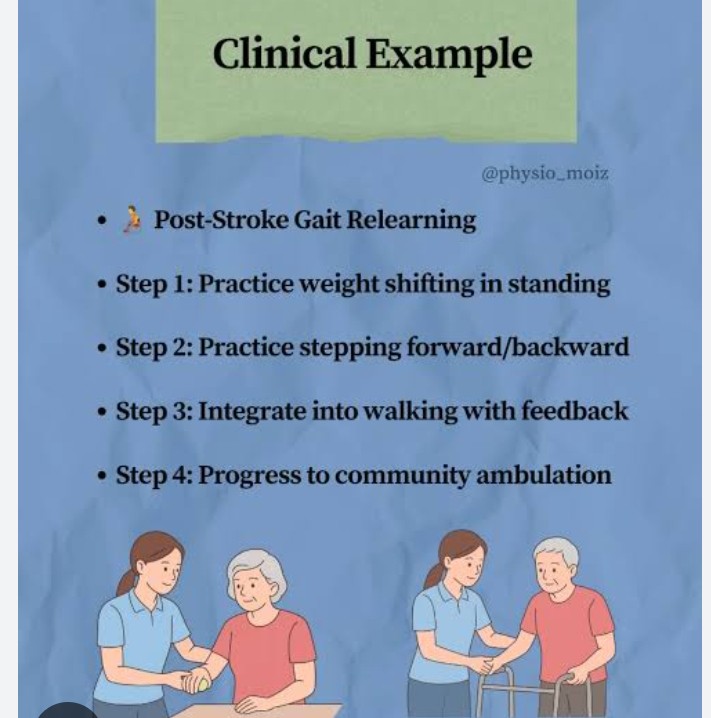
3. PRACTICE OF TASK:
Transition from cognitive to automatic phase of learning (overlaps with Step 2)
4. TRANSFERENCE OF LEARNING:
Carry-over of learning into task performance during daily routines.
Strategies for instructing the patient:
Verbal instruction is kept to a minimum.The therapist identifies the most important aspect of the movement on which the patient will concentrate.
Visual demonstration is provided by the therapist’s performance of the task, focusing on one or two most important components.
Manual guidance helps to clarify the model of action by passively guiding the patient through the path of movement or by physically constraining inappropriate components.
Accurate,timely feedback about the quality of performance helps the patient to learn which strategies to repeat and which ones to avoid.
Consistency of practice facilitates development of skill in task performance.