Cervical Radiculopathy Physical Therapy Management
Treatment Options:
Following includes:
Education and Advice:
Manual Therapy – PAIVMs (Passive Assessory.
Intervertebral Movements) / PPIVMs (Passive Physiological Intervertebral Movements) / NAGs (Natural Apophyseal Glides) / SNAGs (Sustained Natural Apophyseal Glides)
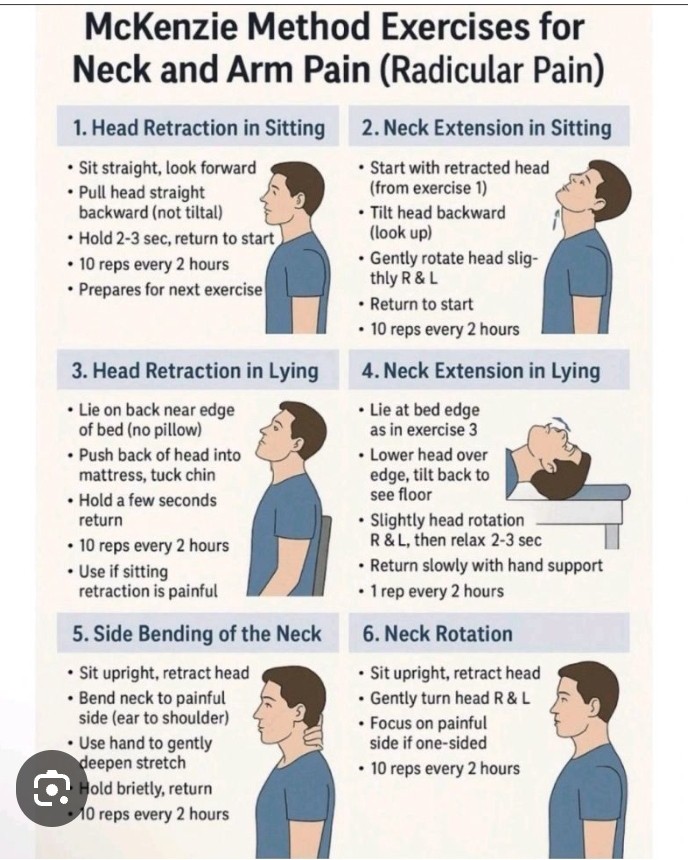
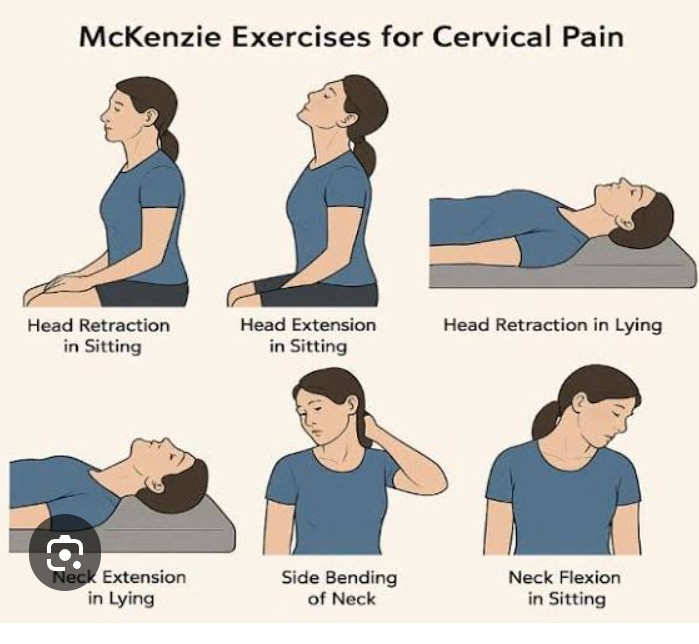
Exercise Therapy – AROM, stretching and strengthening.
Postural Re-education.
Education and Advice:
Education is key to getting the patient on side and to work co-operatively with physiotherapy.If a patient understands the condition and the reason for the neck and arm pain then they are more likely to be compliant with any rehabilitation plan.
In cases of a prolapsed disc, tobacco smoking causes constriction of the vascular network surrounding the intervertebral disc (IVD), reducing the indirect exchange of nutrients and anabolic agents from the blood vessels to the disc improvements in disc health suggesting that,besides quitting smoking, additional treatments should be implemented in the attempt to recover the health of an IVD degenerated by tobacco smoking.
Manual Therapy:
There are some contradictions for using manual therapy techniques and its efficacy is questioned.Reported mobilisation and/or manipulation when combined with exercise was beneficial for pain relief and improvement of function for persistent mechanical neck disorders with or without headache.
Furthermore,cervical spine manipulation carries a risk of complications like vertebral dissection and spinal cord compression because of massive disc herniation.
Therefore,this intervention should be discouraged in cervical radiculopathy, especially if imaging of the spine has not yet been performed.
Aware of any potential risk factors such as arterial insufficiency,Hypertension, Craniovertebral ligament insufficiency and upper motor neurone disorders is also essential.
Fritz JM et al examined the effectiveness of cervical traction in addition to exercise in patients with cervical radiculopathy.Adding mechanical traction to exercise for patients with cervical radiculopathy resulted in lower disability and pain, particularly at long-term follow-ups.
Boyles et al however found that manual therapy consisting of thrust mobilisations of the cervical or thoracic spine and cervical non-thrust mobilisations (PA glides/Lateral Glides in ULTT1 position/Rotations/Retractions) was shown to be effective at reducing pain levels, improving function and increasing joint ROM.
When combined with exercise therapy it was more effective than the control group of manual therapy or exercise therapy however both control groups were effective at reducing signs and symptoms.