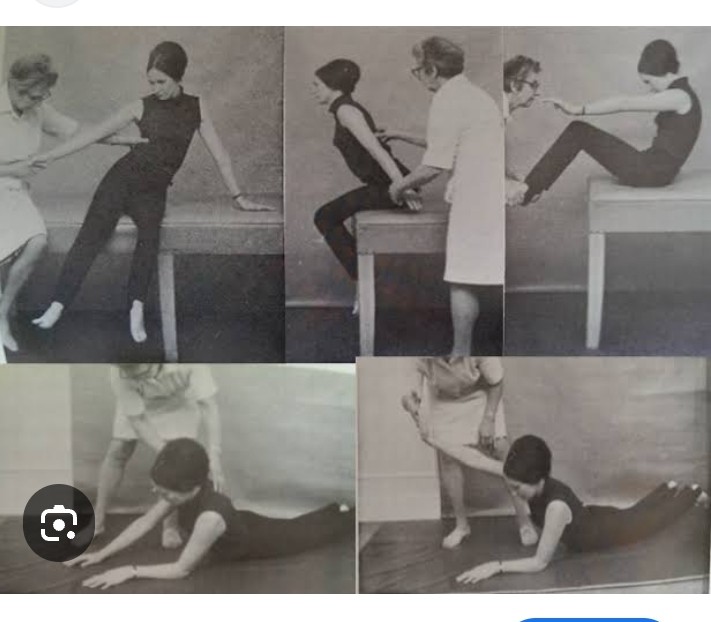
Sitting balance:
Head and trunk movements
Sitting on a firm surface, hands in lap,feet and knees approximately 15 cm
apart, feet on floor.
Turning head and trunk to look over the shoulder, returning to mid position and repeating to other side.
Check:
• Ensure patient rotates the trunk and head, with trunk erect, and remains
flexed at the hips.
• Provide visual targets, increasing the distance to be turned.
• Stabilized the affected foot and prevent external rotation and abduction
at the hip if necessary.
• Ensure hands are not used for support and that feet do not move and Looking up at the ceiling and returning to upright.
Check:
• Patient may overbalance backward and is warned to keep upper body
forward over the hips.
UPPER LIMB FUNCTION:
Training of muscle activity at the scapula and shoulder in supine until the patient can control his shoulder girdle in sitting without excessive compensatory movements.
Upper limb movement problems are usually secondary to shortening of soft tissues due to habitual posturing, use of the intact arm to compensate for the affected arm and learned non-use of the affected arm.
MANAGEMENT:
Early active mobilization of the affected arm in functional patterns.
CAUTION:
Soft tissue damage, chronic inflammation and joint stiffness may be caused by inappropriate passive exercises that do not accommodate the normal biomechanical relationship between the humerus and scapula.
Common Problems and Compensatory Responses:
Impaired scapular movement, especially rotation and protraction.
Persistent depression of the shoulder girdle.
Impaired control over the deltoids causing the inability to sustain shoulder abduction and flexion.
Compensation:
Excessive shoulder girdle elevation.
Lateral trunk flexion.
Excessive shoulder internal rotation,elbow flexion and forearm pronation.
Weakness of glenohumeral joint (GHJ) abductors, flexors and external rotators and of supinators has a significant effect on reaching actions.
Weakness of wrist extensors, finger and thumb flexors and extensors,abductors and adductors affect the manipulation of objects.
Sustaining and controlling grip force during grasping and lifting objects is a common problem.
Reaching Actions:
Sitting,reaching to touch objects with the paretic hand: forward (flexing at the hips),sideways (both sides),backward, returning to mid position.
Very weak patients can practise reaching forward with arms
resting on a high table.
Reaching forward: shoulder girdle elevation, lateral flexion of spine,abduction of shoulder with elbow flexion, internal rotation of shoulder and pronation of forearm.
• Pre-grasp:Excessive opening of hand for grasp to compensate.
• Releasing objects: finger extension with wrist flexed due to contracted long
finger flexors,weak wrist extensors; extending thumb at carpometacarpal
joint (CMC) and metacarpophalangeal joint instead of abducting at
CMC.
Movement:
• Grasping: excessive flexor force in compensation for poor control.
In addition, there are three common adaptive sequelae of stroke:
• Use of the non-paretic limb preferentially when active movement is
possible, and subsequent ‘learned non-use’
• habitual posturing of the paretic limb, leading to adaptive length-associated
changes to soft tissues including loss of extensibility and increased stiffness
of muscle.
Standing Balance:
Head and body movements
Standing with feet a few cm apart, look up at ceiling and return to upright position.
Check:
• Ensure standing alignment is preserved, with hips extended while body rotates.
• Disallow foot movement.If necessary put your foot against patient’s foot to stop movement.
Reaching actions:
• Correct tendency to fall back by a reminder to bring hips forward (hip extension beyond neutral) before looking up.
• Disallow foot movement. Standing with feet a few cm apart, turn head and body mass and look behind,return to mid position, repeat to other side.
Check:
Standing, reaching to take object forward, sideways (both sides),backward.One hand, both hands.Variety of objects and tasks.Reaches should be
beyond arm’s length, challenging the patient to extend the limit of stability and return.
Check:
• Ensure movement of body mass takes place at the ankles and hips, not just within the trunk.
• Discourage a stiff posture and breath holding – encourage relaxed movement.
Single leg support (with or without harness or splint)
Stepping forward with non-paretic limb to place foot on a step.
Standing with either foot on step, practise reaching tasks.
Check:
• Ensure that the stance hip extends. Exercise can be practised initially in a harness.
Note
• Laufer et al. (2000) have shown that stepping forward on to a step of different heights with the non-paretic leg significantly increases weight borne through the paretic limb.
• The exercise directs attention to the concrete goal of raising the leg rather than the more abstract goal of shifting body mass.
Sideways walking:
This exercise enables practice of shifting weight from side to side with hips extended.
Picking up objects:
Standing, lowering body mass to pick up or touch object, forward, sideways,
backward and return.
Check:
• Ensure that hips, knees and ankles flex and extend.
• Start with object on stool to minimize distance to be moved (see Fig. 2.17c).
• Increase flexibility by changing base of support.
Action Reaching :
Forward: flexion at GH joint*
Sideways: abduction at GH joint*
Backward: extension at GH joint* with
– elevation of shoulder girdle
– external rotation at GH joint
– extension of elbow
– supination and pronation of forearm
– extension at wrist
Grasping:
Extension of wrist and fingers, with abduction and conjunct
rotation (‘opposition’) of the CMC joint of thumb and 5th finger.
Flexion of fingers and thumb around object.
Releasing:
Extension at wrist.
Extension at MCP joint of fingers.
Abduction and extension at CMC joint of thumb.
Manipulation:
Flexion and extension of MCP joints of fingers with wrist in
extension.
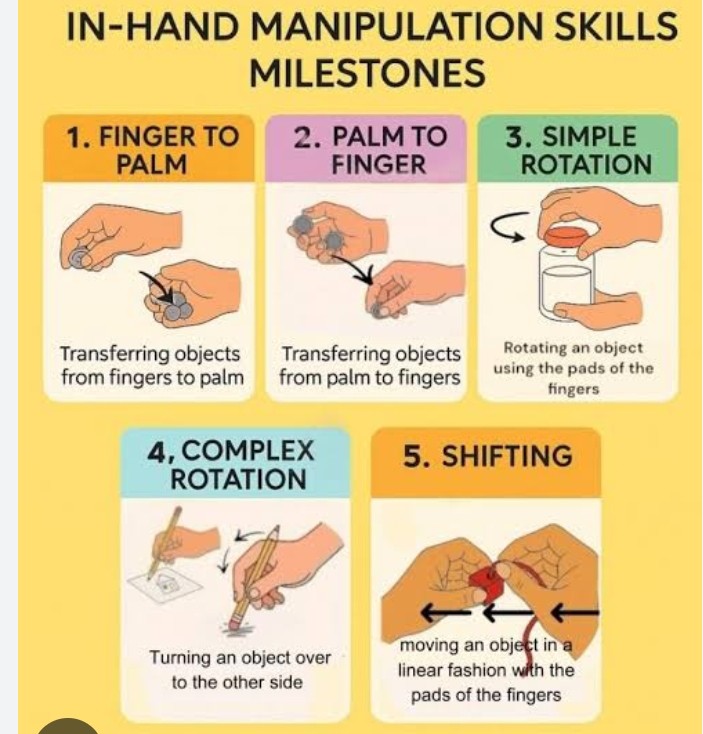
Palmar abduction and conjunct rotation of CMC joint of thumb.
Combined flexion and conjunct rotation at CI”IC joints of 5th
finger and thumb (e.g. cupping)
Independent finger flexion and extension (e.g. tapping)
Key grasp configurations, for example thumb-index; thumb-5th finger; 4th, 5th finger into palm; thumb + flexed MCP, extended interphalangeal (IP) joints of fingers (paper-holding grasp)